Page History
Demographic | Best Practice |
Data Mapping | |
Gender | Open > Demographics screen > Sex
|
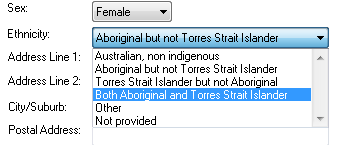
Ethnicity | Open > Demographics screen |
>Drop down list for Aboriginal / TSI
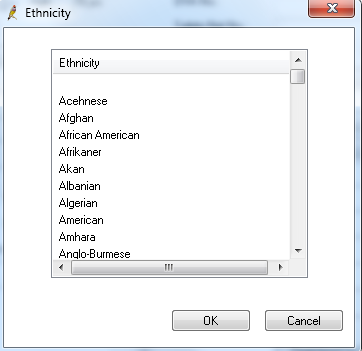
When 'Other' is chosen, BP gives additional options for ethnicity. Only one option can be chosen:
| |
DVA | Open > Demographics screen > DVA No. has a value
|
Age | Open > Demographics screen > DOB
|
Last Visit / Activity |
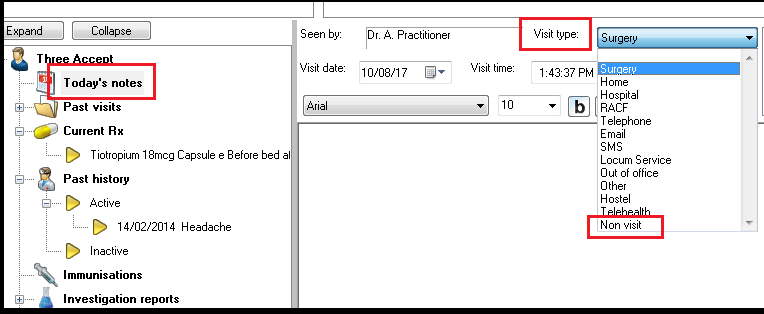
After entering notes on the 'Today's notes' tab, the visit will appear on the 'Past Visits' tab CAT will check the most recent date in the list |
Visits flagged as Type = Non Visit are excluded. |
Last Visit = the most recent date recorded Active = 3 or more visits recorded in the last 2 years |
Note: The past visits screen in Best Practice can be used by practices to record non clinical contacts, for example, when a recall letter is sent. These contacts must be flagged a type Non Visit to be excluded by CAT. |
| |
Postcode | Open > Demographics screen > Postcode |
Allergy
Family History | Main Patient Screen > Family & Social History any information entered on this form will be counted as family history information |
Allergy |
Best Practice Mapping
| Main Patient Screen > Allergies / Adverse Drug Reactions Box | |
Allergy Recorded | An Allergy Item is present |
| |
No Known Allergies | The ‘Nil Known’ check box is checked |
Nothing Recorded | No Allergy Items are present and the ‘Nil Known’ check box is unchecked |
Smoking |
Best Practice Mapping
Main Patient screen > Open > Alcohol and Smoking History > Tobacco |
| Smoking Cessation | Patient would like cessation advice yes/no will be mapped to:
|
Daily Smoker | Smoker = Smoker is selected |
Irregular Smoker | This option is not captured in Best Practice |
Ex Smoker | Smoker = Ex-Smoker is selected |
Never Smoked | Smoker = Never smoked is selected |
Nothing Recorded | Smoker has nothing selected |
Review Date | This will be the date something in the ‘Family & Social History’ section is changed. It is not possible to isolate Smoking changes. |
Alcohol |
Best Practice Mapping
Main Patient screen > Open > Alcohol and Smoking History > Alcohol |
Frequency = days a week patient usually drinks alcohol |
Drinker | Frequency = any except Never |
Non Drinker | Frequency = Never |
Nothing Recorded | Alcohol tab has nothing selected |
Review Date | This will be the date something in the ‘Family & Social History’ section is changed. It is not possible to isolate Alcohol changes. |
Measurements /Pathology * | Best Practice Mapping |
BMI | Patient Record >Main Patient Screen > Observations screen
|
Waist | Patient Record >Main Patient Screen > Observations screen
|
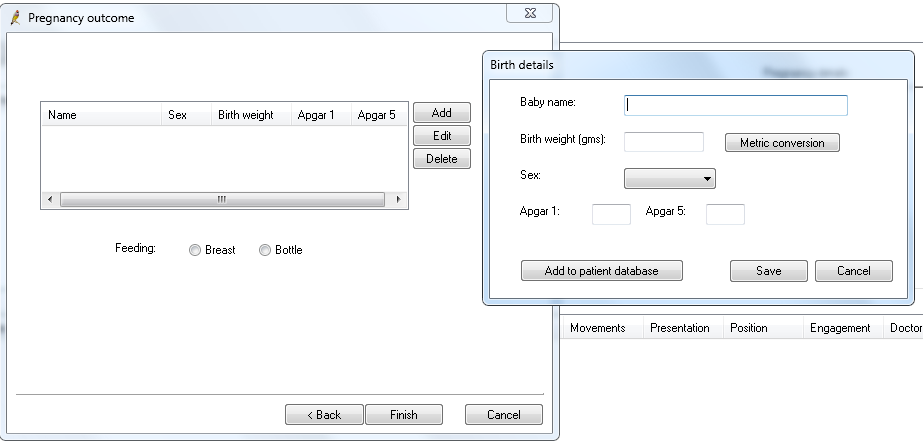
| Birth weight | For the Maternal Health Care report, CAT can extract the birth weight of the child from two sources. One is the child's record, which needs the weight entered and the date backdated to the child's birthday - this will be picked up under the 'Patient Record' report. For the Mother's Antenatal report the birth weight of the child has to be recorded in the mother's record. Under the 'Past Pregnancy' on the 'Obstetric History' tab after adding the pregnancy outcome, BP will show a field for the birth weight of the child born.
|
BSLF | Patient Record >Main Patient Screen > Observations screen OR Patient Record > Main Patient screen > Enhanced Primary Care > Diabetes Cycle of Care screen. OR Pathology HL7 results with LOINC codes 14771-0, 14996-3
|
Cholesterol | Lipids data : Patient Record > Main Patient screen > Enhanced Primary Care > Diabetes Cycle of Care screen. OR Pathology HL7 results OR manually entered result
|
HDL | |
LDL | |
Triglycerides | |
Creatinine | Patient Record > Main Patient screen > Enhanced Primary Care > Diabetes Cycle of Care screen. OR Pathology HL7 results OR manually entered result
|
Urinary creatinine | Pathology HL7 results with LOINC code 14683-7
|
Microalbumin | Patient Record > Main Patient screen > Enhanced Primary Care > Diabetes Cycle of Care screen. OR Pathology HL7 results
|
ACR (Microalbumin Creatinine Ratio)
| Listed in the BP database as an ACR result (with the BP pathology code 17) OR one of these LOINC codes: 32294-1,30000-4,9318-7,14959-1 OR one of these result names: Alb/Cre, Alb/Creat, Albumin/Creatinine, Albumin/Creatinine Ratio, Urinary Albumin/Creatinine Ratio, Urinary Albumin/Creat Ratio, Microalbumin Ratio OR manually entered result
|
HbA1c | Patient Record > Main Patient screen > Enhanced Primary Care > Diabetes Cycle of Care screen. OR Pathology HL7 results OR manually entered result OR Additional test name ‘Blood haemoglobin A 1 c’ |
BP | Patient Record > Main Patient screen either - opening the Observations screen, or - opening the Enhanced Primary Care > Diabetes Cycle of Care screen.
|
Respiratory - Spirometry | Clinical > Respiratory function OR |
Today’s Notes >History and Examination > Respiratory > Calculator > FEV1 and FVC |
|
INR
| Clinical > INR Manager |
Physical Activity | Clinical > Physical Activity Prescription The prescription must be printed for it to be saved. A selected ‘current physical activity level’ of moderate or active meets the physical activity guidelines, otherwise they do not meet the guidelines. We report Inactive as sedentary, Moderate and Active as sufficient.
|
FOBT
| Pathology HL7 results with LOINC code 2335-8, 27396-1, 14563-1, 14564-9, 14565-6, 12503-9, 12504-7, 27401-9, 27925-7, 27926-5, 57905-2,56490-6,56491-4,29771-3
|
FOBT Orders
), OCB NATIONAL SCREENING, FHB, FAECAL BLOOD, %FOBT%, %OCCULT%, Faecal Immunochemical Test, |
The % indicates a wild card search which will pick up any test name with FOBT or OCCULT in the name. | |
eGFR
| Pathology HL7 results with LOINC code 33914-3 OR Calculation (Refer Clinical Audit User Guide – Part 2 Functionality)
|
Pap Smear | Best Practice Mapping |
| Female Patient Record > Main Patient Screen > Cervical Smears tab (Manual entry or Pathology HL7 results) |
Recorded | A smear test is listed |
Smear Date | Date of most recent entry |
Best Practice Pap Smear HL7 Mapping TEST NAME
Best Practice automatically recognises HL7 items as pap smear results if they are this list.
| CCSR CERVICAL CONVENTIONAL SMEAR CERVICAL CYTOLOGY CERVICAL SMEAR CERVICAL SMR CYTOLOGY GYNAECOLOGICAL CYTOLOGY GYNAECOLOGICAL (PAP-0) GYNAE CYTOLOGY GYNAECOLOGICAL CYTOLOGY GYNEA CYTOLOGY NON SCREENING PAP NON SCREENING SMEAR PAN-O PAP PAP (BALLARAT) PAP (GEELONG) PAP NS PAP SMEAR PAP SMEAR (PAN-0) PAP SMEAR +/- THIN PREP PAP SMEAR OLD PAP SMEARS PAP TEST PAP-0 (PAP SMEAR) PAPFU PAPR PAPR NS THIN PREP ONLY THINP VAG SM VAGINAL SMR VAULT CYTOLOGY VAULT SMEAR
Practices should check the test names appearing in the results tab and advise PCS if there is a test name that should be added to this list. |
Pap Smear Ineligible | Best Practice Mapping |
|
Cervical Smears screen - tick-box ‘Not Required’ checked |
Coded condition of Hysterectomy: |
-See Appendix B-1-ii – Screening exclusions
Disease
Best Practice Mapping
Condition
Past History screen > Checks the condition selected on history items, where Conditions are selected from a coded list.
Refer to Appendix C-1 for a list of conditions mapping to each CAT condition.
Medications
Best Practice Mapping
Medication
Current Rx screen > Checks the Drugs listed as current medications, where Drugs are selected from a coded list.
Refer to Appendix C-2 for a list of medications mapping to each CAT medication.
Medication Count
Current Rx screen > Counts All Drugs listed as current medications
Demographic
Best Practice Mapping
Gender
Open > Demographics screen > Sex
Ethnicity
Open > Demographics screen >
Drop down list for Aboriginal / TSI
DVA
Open > Demographics screen > DVA No. has a value
Age
Open > Demographics screen > DOB
Last Visit / Activity
Visits flagged as Type = Non Visit are excluded.
Last Visit = the most recent date recorded
Active = 3 or more visits recorded in the last 2 years
Note: The past visits screen in Best Practice can be used by practices to record non clinical contacts, for example,
when a recall letter is sent. These contacts must be flagged a type Non Visit to be excluded by CAT.
Postcode
Open > Demographics screen > Postcode
Allergy
Main Patient Screen > Allergies / Adverse Drug Reactions Box
Allergy Recorded
An Allergy Item is present
No Known Allergies
The 'Nil Known' check box is checked
Nothing Recorded
No Allergy Items are present and the 'Nil Known' check box is unchecked
Smoking
Main Patient screen > Open > Alcohol and Smoking History > Tobacco
Daily Smoker
Smoker = Smoker is selected
Irregular Smoker
This option is not captured in Best Practice
Ex Smoker
Smoker = Ex-Smoker is selected
Never Smoked
Smoker = Never smoked is selected
Nothing Recorded
Smoker has nothing selected
Review Date
This will be the date something in the 'Family & Social History' section is changed.
It is not possible to isolate Smoking changes.
Alcohol
Main Patient screen > Open > Alcohol and Smoking History > Alcohol
Frequency = days a week patient usually drinks alcohol
Drinker
Frequency = any except Never
Non Drinker
Frequency = Never
Nothing Recorded
Alcohol tab has nothing selected
Review Date
This will be the date something in the 'Family & Social History' section is changed.
It is not possible to isolate Alcohol changes.
Measurements
*/Pathology **
Best Practice Mapping
BMI
Patient Record >Main Patient Screen > Observations screen
Waist
Patient Record >Main Patient Screen > Observations screen
BSLF
Patient Record >Main Patient Screen > Observations screen
OR
Patient Record > Main Patient screen > Enhanced Primary Care > Diabetes Cycle of Care screen.
OR
Pathology HL7 results with LOINC codes 14771-0, 14996-3
Cholesterol
Lipids data :
Patient Record > Main Patient screen > Enhanced Primary Care > Diabetes Cycle of Care screen.
OR
Pathology HL7 results
OR manually entered result
HDL
LDL
Triglycerides
Creatinine
Patient Record > Main Patient screen > Enhanced Primary Care > Diabetes Cycle of Care screen.
OR
Pathology HL7 results
OR manually entered result
Urinary creatinine
Pathology HL7 results with LOINC code 14683-7
Microalbumin
Patient Record > Main Patient screen > Enhanced Primary Care > Diabetes Cycle of Care screen.
OR
Pathology HL7 results
ACR (Microalbumin Creatinine Ratio)
Listed in the BP database as an ACR result (with the BP pathology code 17)
OR one of these LOINC codes: 32294-1,30000-4,9318-7,14959-1
OR one of these result names: Alb/Cre, Alb/Creat, Albumin/Creatinine, Albumin/Creatinine Ratio,
Urinary Albumin/Creatinine Ratio, Urinary Albumin/Creat Ratio, Microalbumin Ratio
OR manually entered result
HbA1c
Patient Record > Main Patient screen > Enhanced Primary Care > Diabetes Cycle of Care screen.
OR
Pathology HL7 results
OR manually entered result
OR
Additional test name 'Blood haemoglobin A 1 c'
BP
Patient Record > Main Patient screen either
- opening the Observations screen, or
- opening the Enhanced Primary Care > Diabetes Cycle of Care screen.
Respiratory - Spirometry
OR
Today's Notes >History and Examination > Respiratory > Calculator > FEV1 and FVC
INR
Clinical > INR Manager
Physical Activity
Clinical > Physical Activity Prescription
The prescription must be printed for it to be saved.
A selected 'current physical activity level' of moderate or active meets the physical activity guidelines, otherwise they do not meet the guidelines
FOBT
or with test names Faecal Occult Blood ,Faecal occult blood screening ,Faecal Occult Blood Test, FOB, FOBT, Occult blood – faeces,
Stool occult blood test, OCCULT BLOOD, faecal human haemoglobin,Insure FOBT, FOBT1, FOBT2, FOBT3, FOB1, FOB2, FOB3, BOW,
OCCULT BLOOD (OCB-0), OCCULT BLOOD (OCB-1), OCCULT BLOOD (OCB-2
FOBT Orders are extracted with any of the test names above.
eGFR
Pathology HL7 results with LOINC code 33914-3
OR
Calculation (Refer Clinical Audit User Guide – Part 2 Functionality)
* Refer to pathology note at the start of this manual and Appendix
Pap Smear
Best Practice Mapping
Female Patient Record >
Main Patient Screen > Cervical Smears tab
(Manual entry or Pathology HL7 results)
Recorded
A smear test is listed
Smear Date
Date of most recent entry
TEST NAME
Best Practice automatically recognises HL7 items as pap smear results if they are this list.CCSR
CERVICAL CONVENTIONAL SMEAR
CERVICAL CYTOLOGY
CERVICAL SMEAR
CERVICAL SMR
CYTOLOGY GYNAECOLOGICAL
CYTOLOGY GYNAECOLOGICAL (PAP-0)
GYNAE CYTOLOGY
GYNAECOLOGICAL CYTOLOGY
GYNEA CYTOLOGY
NON SCREENING PAP
NON SCREENING SMEAR
PAP
PAP (BALLARAT)
PAP (GEELONG)
PAP NS
PAP SMEAR
PAP SMEAR (PAN-0)
PAP SMEAR +/- THIN PREP
PAP SMEAR OLD
PAP SMEARS
PAP TEST
PAP-0 (PAP SMEAR)
PAPFU
PAPR
PAPR NS
THIN PREP ONLY
THINP
VAG SM
VAGINAL SMR
VAULT CYTOLOGY
VAULT SMEAR
Practices should check the test names appearing in the results tab and
advise PCS if there is a test name that should be added to this list.
Pap Smear Ineligible
Best Practice Mapping
2) Coded condition of Hysterectomy:
-See Appendix B-1-ii – Screening exclusions
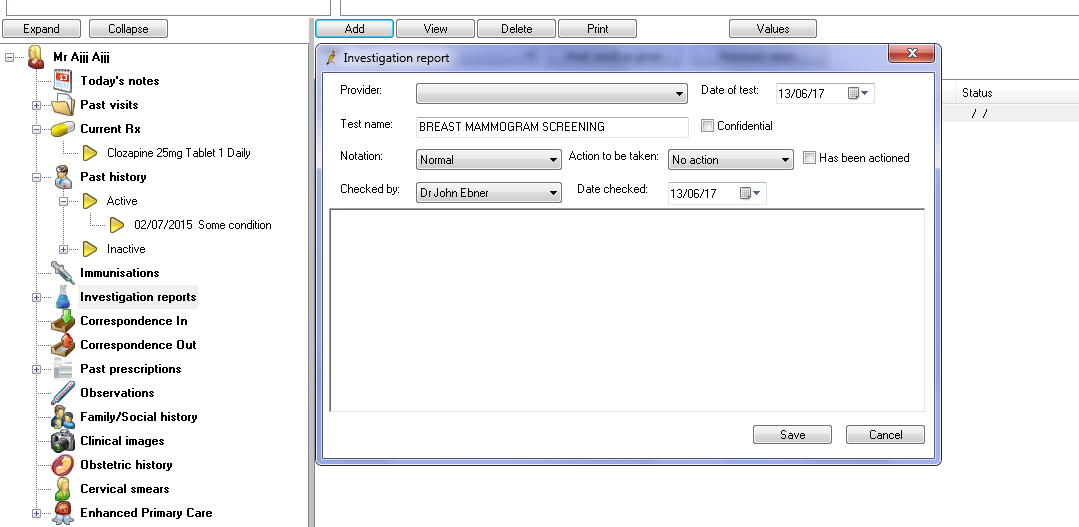
| Mammogram |
Mammogram results are not sent electronically in all states, but if test names are entered manually into the results tab CAT4 will pick up that the test has been done. The following test names are recognised:
To manually add a mammogram result click on the 'Add' button under the 'Investigation report' tab, then enter one of the test names from above and complete the other fields. CAT4 will only extract the test name and date but no outcome/result.
|
Disease | Best Practice Mapping |
Condition | Past History screen > Checks the condition selected on history items, where Conditions are selected from a coded list.
Refer to Appendix C-1 for a list of conditions mapping to each CAT condition.
|
Medications | Best Practice Mapping |
Medication | Current Rx screen > Checks the Drugs listed as current medications, where Drugs are selected from a coded list.
Refer to Appendix C-2 for a list of medications mapping to each CAT medication.
|
Medication Count | Current Rx screen > Counts All Drugs listed as current medications
|
...
Demographic
...
Best Practice Mapping
...
Gender
...
Open > Demographics screen > Sex
...
Ethnicity
...
Open > Demographics screen >
Drop down list for Aboriginal / TSI
...
DVA
...
Open > Demographics screen > DVA No. has a value
...
Age
...
Open > Demographics screen > DOB
...
Last Visit / Activity
...
Past Visits screen > Checks most recent date in the list
Visits flagged as Type = Non Visit are excluded.
Last Visit = the most recent date recorded
Active = 3 or more visits recorded in the last 2 years
Note: The past visits screen in Best Practice can be used by practices to record non clinical contacts, for example, when a recall letter is sent. These contacts must be flagged a type Non Visit to be excluded by CAT.
...
Postcode
...
Open > Demographics screen > Postcode
...
Allergy
...
Best Practice Mapping
Main Patient Screen > Allergies / Adverse Drug Reactions Box
...
Allergy Recorded
...
An Allergy Item is present
...
No Known Allergies
...
The ‘Nil Known’ check box is checked
...
Nothing Recorded
...
No Allergy Items are present and the ‘Nil Known’ check box is unchecked
...
Smoking
...
Best Practice Mapping
Main Patient screen > Open > Alcohol and Smoking History > Tobacco
...
...
Daily Smoker
...
Smoker = Smoker is selected
...
...
Irregular Smoker
...
This option is not captured in Best Practice
...
...
Ex Smoker
...
Smoker = Ex-Smoker is selected
...
...
Never Smoked
...
Smoker = Never smoked is selected
...
...
Nothing Recorded
...
Smoker has nothing selected
...
...
Review Date
...
This will be the date something in the ‘Family & Social History’ section is changed. It is not possible to isolate Smoking changes.
...
...
Alcohol
...
Best Practice Mapping
Main Patient screen > Open > Alcohol and Smoking History > Alcohol
Frequency = days a week patient usually drinks alcohol
...
...
Drinker
...
Frequency = any except Never
...
...
Non Drinker
...
Frequency = Never
...
...
Nothing Recorded
...
Alcohol tab has nothing selected
...
...
Review Date
...
This will be the date something in the ‘Family & Social History’ section is changed. It is not possible to isolate Alcohol changes.
...
...
Measurements
/Pathology *
...
Best Practice Mapping
...
...
BMI
...
Patient Record >Main Patient Screen > Observations screen
...
...
Waist
...
Patient Record >Main Patient Screen > Observations screen
...
...
BSLF
...
Patient Record >Main Patient Screen > Observations screen
OR
Patient Record > Main Patient screen > Enhanced Primary Care > Diabetes Cycle of Care screen.
OR
Pathology HL7 results with LOINC codes 14771-0, 14996-3
...
...
Cholesterol
...
Lipids data :
Patient Record > Main Patient screen > Enhanced Primary Care > Diabetes Cycle of Care screen.
OR
Pathology HL7 results
OR manually entered result
...
...
HDL
...
...
LDL
...
...
Triglycerides
...
...
Creatinine
...
Patient Record > Main Patient screen > Enhanced Primary Care > Diabetes Cycle of Care screen.
OR
Pathology HL7 results
OR manually entered result
...
...
Urinary creatinine
...
Pathology HL7 results with LOINC code 14683-7
...
...
Microalbumin
...
Patient Record > Main Patient screen > Enhanced Primary Care > Diabetes Cycle of Care screen.
OR
Pathology HL7 results
...
...
ACR (Microalbumin Creatinine Ratio)
...
Listed in the BP database as an ACR result (with the BP pathology code 17)
OR one of these LOINC codes: 32294-1,30000-4,9318-7,14959-1
OR one of these result names: Alb/Cre, Alb/Creat, Albumin/Creatinine, Albumin/Creatinine Ratio, Urinary Albumin/Creatinine Ratio, Urinary Albumin/Creat Ratio, Microalbumin Ratio
OR manually entered result
...
...
HbA1c
...
Patient Record > Main Patient screen > Enhanced Primary Care > Diabetes Cycle of Care screen.
OR
Pathology HL7 results
OR manually entered result
OR
Additional test name ‘Blood haemoglobin A 1 c’
...
...
BP
...
Patient Record > Main Patient screen either
- opening the Observations screen, or
- opening the Enhanced Primary Care > Diabetes Cycle of Care screen.
...
...
Respiratory - Spirometry
...
Clinical > Respiratory function
OR
Today’s Notes >History and Examination > Respiratory > Calculator > FEV1 and FVC
...
...
INR
...
Clinical > INR Manager
...
...
Physical Activity
...
Clinical > Physical Activity Prescription
The prescription must be printed for it to be saved.
A selected ‘current physical activity level’ of moderate or active meets the physical activity guidelines, otherwise they do not meet the guidelines
...
...
FOBT
...
Pathology HL7 results with LOINC code 2335-8, 27396-1, 14563-1, 14564-9, 14565-6, 12503-9, 12504-7, 27401-9, 27925-7, 27926-5
or with test names Faecal Occult Blood ,Faecal occult blood screening ,Faecal Occult Blood Test, FOB, FOBT, Occult blood – faeces, Stool occult blood test, OCCULT BLOOD, faecal human haemoglobin,Insure FOBT, FOBT1, FOBT2, FOBT3, FOB1, FOB2, FOB3, BOW, OCCULT BLOOD (OCB-0), OCCULT BLOOD (OCB-1), OCCULT BLOOD (OCB-2
FOBT Orders are extracted with any of the test names above.
...
...
eGFR
...
Pathology HL7 results with LOINC code 33914-3
OR
Calculation (Refer Clinical Audit User Guide – Part 2 Functionality)
...
...
Pap Smear
...
Best Practice Mapping
...
...
...
Female Patient Record >
Main Patient Screen > Cervical Smears tab
(Manual entry or Pathology HL7 results)
...
...
Recorded
...
A smear test is listed
...
...
Smear Date
...
Date of most recent entry
...
...
Best Practice Pap Smear HL7 Mapping
TEST NAME
Best Practice automatically recognises HL7 items as pap smear results if they are this list.
...
CCSR
CERVICAL CONVENTIONAL SMEAR
CERVICAL CYTOLOGY
CERVICAL SMEAR
CERVICAL SMR
CYTOLOGY GYNAECOLOGICAL
CYTOLOGY GYNAECOLOGICAL (PAP-0)
GYNAE CYTOLOGY
GYNAECOLOGICAL CYTOLOGY
GYNEA CYTOLOGY
NON SCREENING PAP
NON SCREENING SMEAR
PAP
PAP (BALLARAT)
PAP (GEELONG)
PAP NS
PAP SMEAR
PAP SMEAR (PAN-0)
PAP SMEAR +/- THIN PREP
PAP SMEAR OLD
PAP SMEARS
PAP TEST
PAP-0 (PAP SMEAR)
PAPFU
PAPR
PAPR NS
THIN PREP ONLY
THINP
VAG SM
VAGINAL SMR
VAULT CYTOLOGY
VAULT SMEAR
Practices should check the test names appearing in the results tab and advise PCS if there is a test name that should be added to this list.
...
...
Pap Smear Ineligible
...
Best Practice Mapping
...
...
...
1) Cervical Smears screen - tick-box ‘Not Required’ checked
2) Coded condition of Hysterectomy:
-See Appendix B-1-ii – Screening exclusions
...
...
Disease
...
Best Practice Mapping
...
...
Condition
...
Past History screen > Checks the condition selected on history items, where Conditions are selected from a coded list.
Refer to Appendix C-1 for a list of conditions mapping to each CAT condition.
...
...
Medications
...
Best Practice Mapping
...
...
Medication
...
Current Rx screen > Checks the Drugs listed as current medications, where Drugs are selected from a coded list.
Refer to Appendix C-2 for a list of medications mapping to each CAT medication.
...
...
Medication Count
...
| My Health Record status | To update a patient's MHR status from unknown the 'My Health Record' menu needs to be accessed in BP. If no one has clicked on 'My Health Record' then CAT4 will list the status as 'unknown'.
|

* Refer to pathology note at the start of this manual and Appendix